
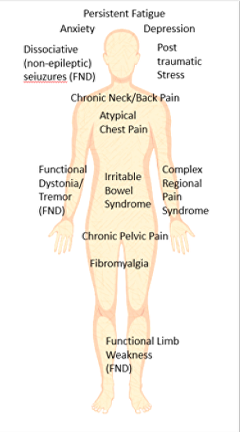
Studies have shown that people with FND have a higher frequency of experiencing functional symptoms elsewhere in the body.
These may include:
Irritable Bowel Syndrome
Unexplained heartburn and indigestion (functional dyspepsia)
Fibromyalgia (see pain)
Temporomandibular Joint Dysfunction
Atypical Facial Pain
Loin Pain Haematuria Syndrome
Chronic Unexplained Fatigue (see fatigue)
Chronic Pelvic Pain
Atypical chest pain
Dysfunctional Breathing
Sometimes, this reflects a very longstanding vulnerability to these symptoms with different symptoms coming and going since late teenage / early twenties.
This is not always the case. You can have any of the functional symptoms described in this website in isolation or you can be very healthy for 40 or 50 years and then get lots of functional symptoms even when you have never had them before.
But it can be useful to see that, if you do find yourself seeing your GP or different specialists with lots of different genuine symptoms and ‘nothing seems to turn up’, that you are not alone and this pattern of illness is well recognised.
This section is here to help ‘join the dots’ between different specialities which tend to only think about their conditions. Its obviously important that the diagnoses below are made by a qualified professional. Don’t assume you have these just because you have FND.
This common condition usually presents with abdominal bloating or pain associated with constipation and/or diarrhoea. Together with other functional abdominal problems it accounts for one third to one half of all patients seen in gastroenterological clinics in hospital As with functional neurological symptoms, there is no structuaral disease process causing the symptoms. Gastroenterologists view IBS as a genuine problem which is caused by a disorder in the function of the gastrointestinal tract. The focus of attention in this condition has been looking at disturbances in the nervous control of the bowel (including the brain).
Irritable Bowel Syndrome has been defined by gastrointestinal specialists as:
At least 3 months, with onset at least 6 months previously of recurrent abdominal pain or discomfort* associated with 2 or more of the following:
• Improvement with defecation; and/or
• Onset associated with a change in frequency of stool; and/or
• Onset associated with a change in form (appearance) of stool
*Discomfort means an uncomfortable sensation not described as pain.
To find out more about IBS visit
The IBS Network – a UK organisation for people with irritable bowel syndrome
The Rome Foundation – an organisation of health professionals involved in functional gastrointestinal disorders
This is when people have heartburn or indigestion symptoms but nothing can be found to explain the symptoms with camera or other tests. Functional dyspepsia has been defined by gastrointestinal specialists as:
At least 3 months, with onset at least 6 months previously, of 1 or more of the following:
• Bothersome postprandial fullness
• Early satiation
• Epigastric pain
• Epigastric burning and
• No evidence of structural disease (including at upper endoscopy) that is likely to explain the symptoms
In women with functional neurological symptoms there is a striking increased frequency of previous gynaecological problems. This may include
• Excessive Period pain
• Heavy periods
• Chronic pelvic pain
As a result of these symptoms, there is a much higher rate of hysterectomy (removal of the womb) in patients with FND than the general population
Whilst there is a clear association with these gynaecological problems, it is not known clearly what lies behind it. A vulnerability to pain symptoms and syndromes may be important. It may be that things that cause pelvic pain such as endometriosis, create the conditions for chronic pain thereafter.
The most useful thing to know here is that if you do have a history of gynaecological trouble and now have FND, then this may not be a complete coincidence.
Men with functional neurological symptoms are also probably more prone to developing testicular pain in the same way, although the literature on this is smaller.
When people present to a chest pain clinic, around one third of patients have no evidence of coronary artery disease, stomach/gullet or other recognised cause for pain. Their pain is all too real though, may be recurrent and be frightening as it feels as if they are having symptoms of angina or a heart attack.
Often this presentation is called ‘atypical chest pain’. It is another functional symptom best thought of as a pain syndrome affecting the chest (see pain). Pain in the chest is alarming. Also, alarm, in the form of acute severe anxiety (called panic), typically causes a feeling of chest tightness. So it is easy to see how these two conditions can make each other worse in a vicious circle.
It is important to recognise that many people with atypical chest pain are not that anxious and do not panic.
People with dysfunctional breathing (breathing too fast and/or too deeply) can have a range of neurological symptoms including dizziness, tingling, tiredness and breathlessness. PEople with dysfunctional breathing often notice that they are breathless or that they take ‘sighing’ respirations. Patients may have a low carbon dioxide in their bloodstream from breathing too much and this exacerbates the symptoms in a physiological way.
Treatment designed at improving breathing, sometimes called breathing retraining, can be very helpful at improving other symptoms.


We will be re-directing you to the University of Edinburgh’s donate page, which enable donations in a secure manner on our behalf. We use donations for keeping the site running and further FND research.
